01 Aug 2018
Author: Maryland Franklin, PhD | Vice President, Scientific Development
Date: August 2018
Triple negative breast cancer (TNBC), accounting for 15-20% of all breast cancers, lacks estrogen receptors, progesterone receptors, and amplification or overexpression of Her-2. As such, these tumors are not responsive to hormonal or anti-Her2 therapies, and are usually treated with combinations of surgery, radiation, and chemotherapy. Although many triple negative tumors respond well to chemotherapy, patients generally have poorer prognosis, higher relapse rates with aggressive tumor growth, and high metastatic potential. More than 300 clinical trials are currently ongoing in TNBC (www.clinicaltrials.gov) evaluating various single agent and combination approaches with chemotherapy, targeted therapy, immunotherapy, and radiation therapy. Clinically, radiation therapy has been associated with decreased risk of locoregional recurrence and some instances of improved overall survival when compared to patients that did not receive radiation therapy.1, 2
Preclinically there are few options to test effects of clinically relevant radiation therapy approaches. Labcorp has a Small Animal Radiation Research Platform (SARRP; Xstrahl) in house and can provide a solution to this currently unmet preclinical need.
HCC70 Evaluation With Paclitaxel and Docetaxel
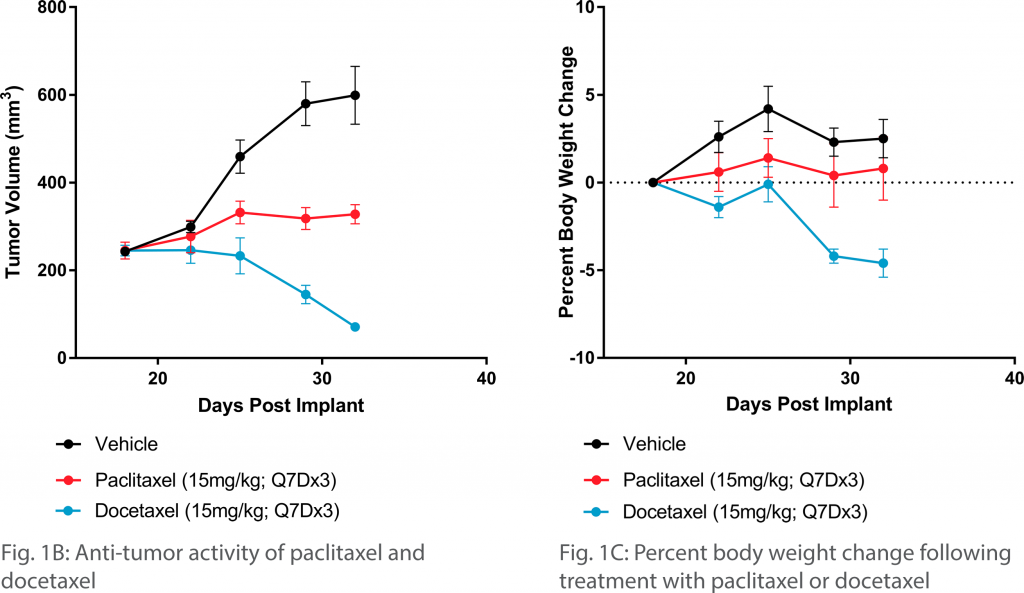
The HCC70 human TNBC cell line can be used to model this disease preclinically. This cell line grows well following subcutaneous implant in female NSG mice (Figure 1A). To determine which chemotherapy would be suitable for combination approaches we evaluated both paclitaxel and docetaxel. We observed a strong response to docetaxel and a more modest response to paclitaxel (Figure 1B) with minimal effects on body weight loss (Figure 1C). The response to paclitaxel was further verified in an additional study (data not shown).
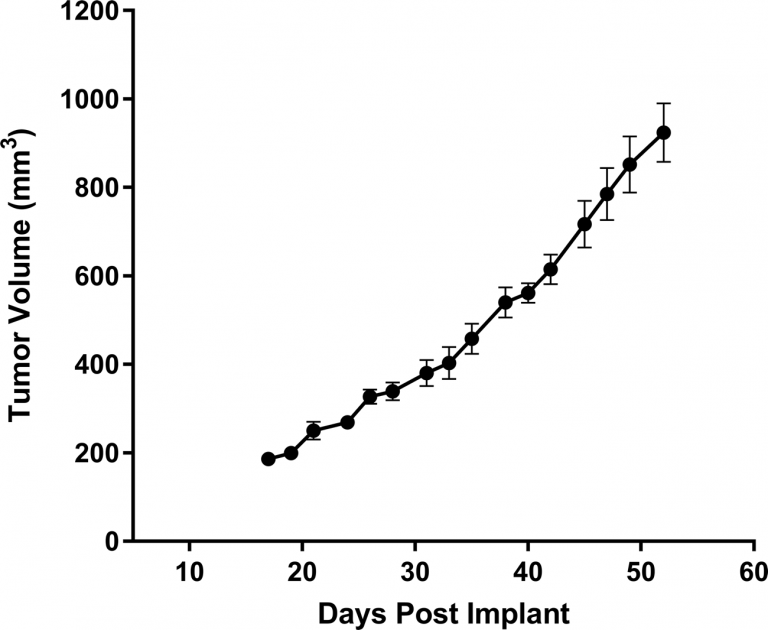
Fig. 1A: Subcutaneous growth of HCC70 in female NSG mice
HCC70 Response to Radiation
To determine the benefit of paclitaxel in combination with focal radiation, we further employed HCC70 tumor bearing mice to investigate both fractionated (2.5Gy given 5 days on and 2 days off for two cycles) and hypofractionated (8Gy for 3 consecutive days only) radiation treatment plans.
The HCC70 tumor model was sensitive to radiation, and we found that hypofractionated radiation resulted in a slightly improved anti-tumor response with a slightly increased toxicity profile, based on body weight loss (Figures 2A and 2B). However, neither radiation treatment resulted in tumor free survivors, only prolonged tumor stasis based on caliper measurements (Table 1).
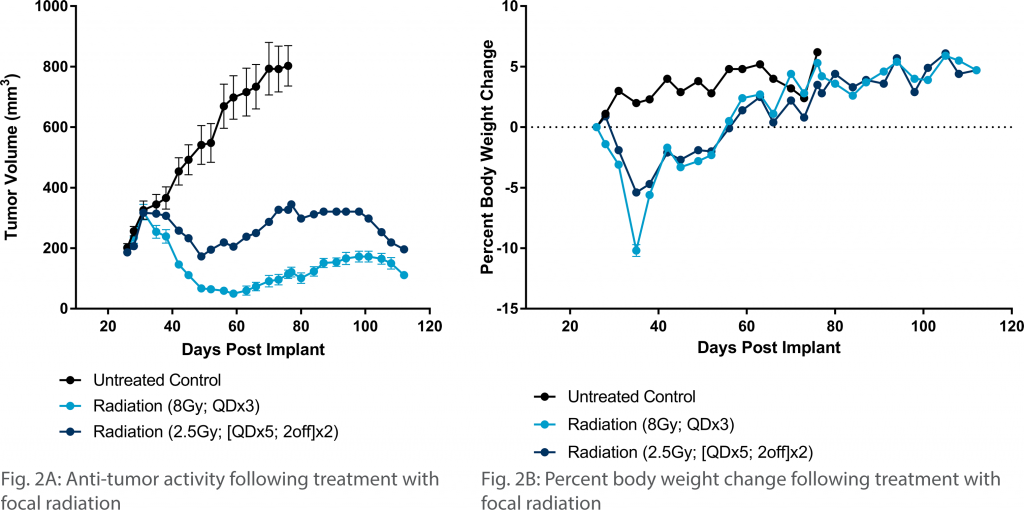
Table 1: Endpoint Analysis Following Treatment with Paclitaxel and Focal Radiation

HCC70 Combination Treatment with Radiation and Paclitaxel
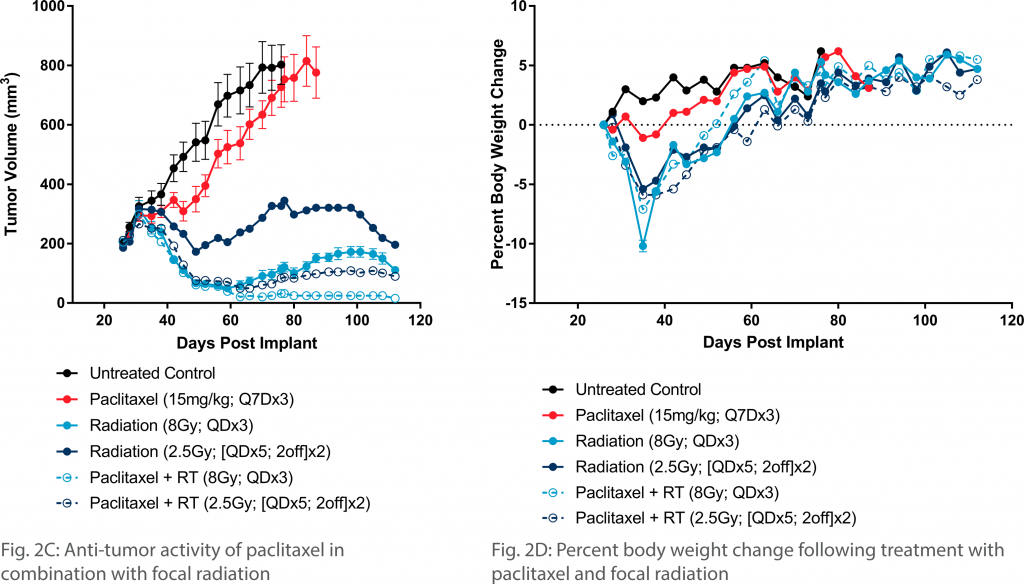
When either radiation regimen was combined with paclitaxel the results were increased anti-tumor activity over monotherapies (Figures 2C). With treatment of fractionated radiation and paclitaxel, we observed 12.5% tumor free survivors and 37.5% complete regressions. This anti-tumor activity was increased to 87.5% tumor free survivors and 87.5% complete regressions when hypofractionated radiation was utilized (Table 1). While the hypofractionated treatment approach resulted in added therapeutic benefit, we did observe increased body weight loss (Figure 2D). Thus, the advantage of hypofractionated radiation comes at the cost of lower tolerability.
Conclusion
HCC70 will be a useful model for those looking to interrogate new and novel treatment approaches for TNBC as well as for those looking to combine with paclitaxel and/or radiation therapy. For related information, see our poster: “Focal Radiation Enhances Paclitaxel Therapy in a Mouse Model of Triple Negative Breast Cancer”